Can J&K’s Private Rehabs Survive the New Rule of Law?
By Ajaz Rashid
The narrow alleys of Srinagar and the bustling suburbs of Jammu have, for decades, played host to a quiet and desperate commerce. Behind non-descript gates and within the confines of residential basements, a proliferation of “de-addiction centers” emerged to meet a soaring demand. Some of these facilities offered genuine lifelines, staffed by dedicated professionals working with limited resources. Others, however, were little more than unregulated warehouses for the broken, operating in a legal vacuum where “treatment” was a loosely defined term and accountability was non-existent. This era of the “wild west” in Jammu & Kashmir’s rehabilitation sector has officially reached its conclusion. In a move that signals a scorched-earth policy against subpar care, the Union Territory administration has unveiled the Jammu & Kashmir Substance Use Disorder Treatment, Counselling and Rehabilitation Centre Rules, 2026. Enacted under the sweeping powers of the Narcotic Drugs and Psychotropic Substances (NDPS) Act, 1985, this legislative framework represents one of the most significant public health interventions in the region’s recent history. It transforms the landscape of substance abuse recovery from a discretionary, often amateur service into a highly regulated, clinically mandated medical necessity.
To understand the weight of these new regulations, one must first look at the staggering scale of the crisis they intend to solve. Recent data suggests that Jammu & Kashmir is a region under siege by narcotics. While official numbers are often debated, internal assessments and surveys by the Ministry of Social Justice and Empowerment have frequently flagged the UT as having one of the highest densities of substance users in northern India. Estimates now suggest that nearly 10 lakh (1 million) individuals across the Union Territory are struggling with some form of substance use disorder, with heroin and synthetic opioids being the primary drivers of this epidemic. This surge in addiction created a massive imbalance between supply and demand. Government facilities, though highly professional, were overwhelmed by waiting lists that stretched for months. This vacuum was filled by private players, many of whom opened centers without any clinical background, driven either by a well-intentioned but amateur desire to help or, in darker cases, by the prospect of profit from desperate families. The 2026 Rules are a direct response to this chaos, designed to separate the healers from the exploiters.

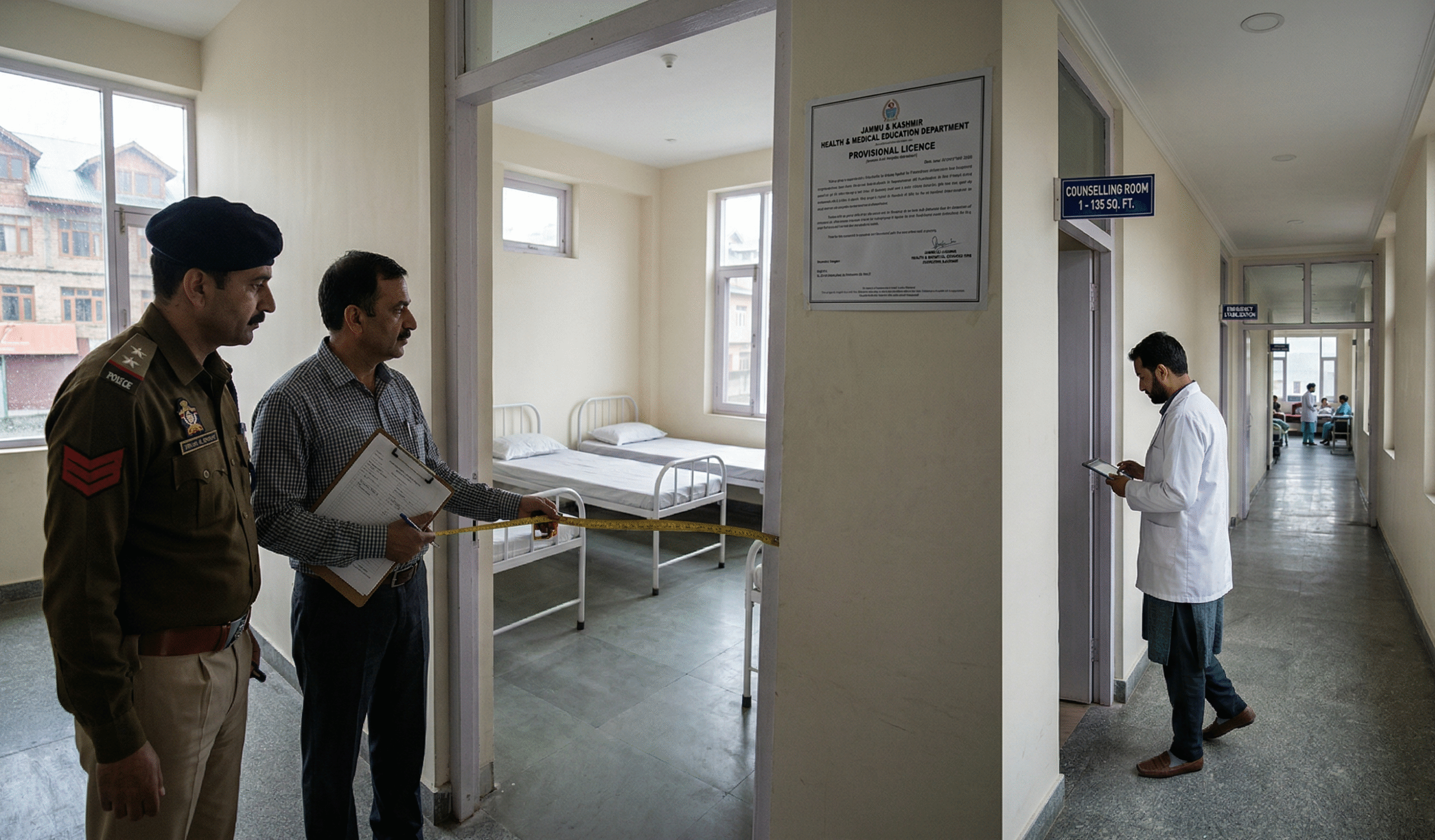
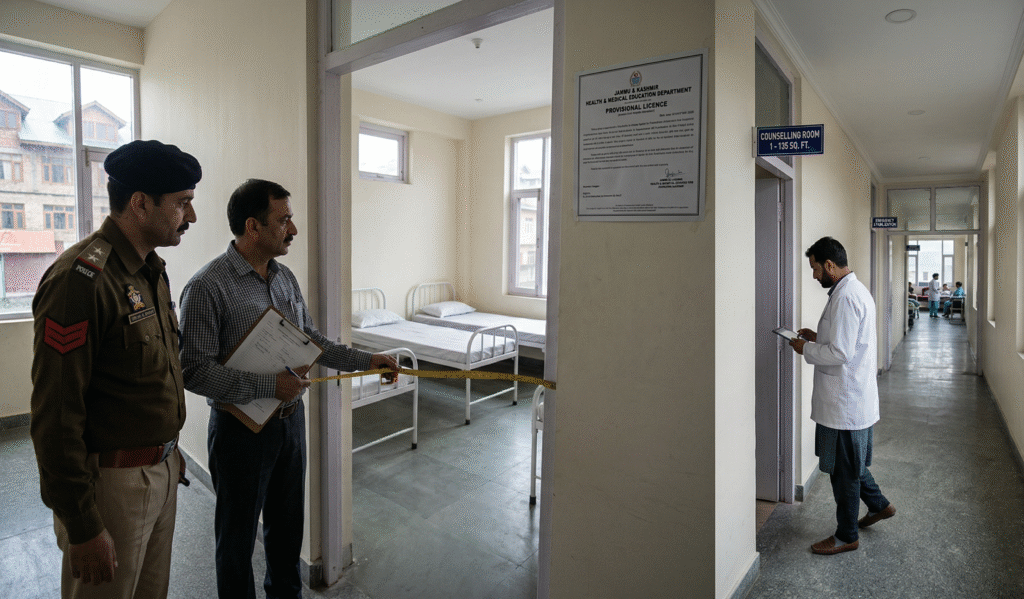
The notification marks the beginning of a ticking clock for every rehabilitation facility in the region. The government has designated the Director of Health Services (Jammu/Kashmir) as the ultimate gatekeeper and licensing authority. The mandate is clear: every existing drug de-addiction and rehabilitation center must apply for a formal license within exactly six months from the issuance of these rules. This is not a mere rubber-stamp exercise. To secure a license, a center must undergo a gauntlet of inspections that evaluate everything from physical infrastructure and staffing ratios to the ethics of their counseling systems and the integrity of their record-keeping. The rules explicitly forbid any person or entity from operating a center without a valid license, effectively criminalizing the unregulated clinics that have operated with impunity for years. By grounding these rules in the NDPS Act, the government has given itself the teeth to shut down non-compliant facilities and prosecute those who jeopardize patient safety.
Perhaps the most culturally significant change is the restriction on where these centers can operate. For years, residents in many neighborhoods have complained about “hidden” clinics operating out of rented houses in quiet cul-de-sacs, often leading to friction between the community and the patients. The 2026 Rules address this head-on: “No Centre shall function in a residential area without prior approval of the Municipal Corporation, Municipality, or Panchayat concerned and shall also obtain a No Objection Certificate (NOC) from the concerned police station.” This clause serves a dual purpose. It ensures that rehabilitation centers are integrated into the community with transparency and safety, but it also acts as a barrier against the “fly-by-night” operations that prefer to stay in the shadows to avoid government scrutiny. By involving local governance and the police in the approval process, the administration is making the community a stakeholder in the recovery process while ensuring that patients are treated in environments that meet civic safety standards.
-
The Ultimatum: All existing de-addiction centers in J&K have a strict six-month deadline to meet new clinical standards or face immediate closure.
-
Digital Watch: Introduction of the Unique Treatment Identification Number (UTIN) to track patient history and prevent the diversion of prescription drugs.
-
Space & Privacy: New mandates require 400 sq. ft. per 10 beds and strictly segregated wards for female patients to ensure dignity in recovery.
-
The Expert Guard: Centers must now employ a fixed ratio of clinical psychiatrists, psychologists, and nurses—moving away from amateur-led “containment.”
-
Community Oversight: Rehab facilities are banned from residential areas unless they secure explicit clearance from local Panchayats and the police.
The physical blueprint for healing has also been radically redefined. The government has moved away from vague guidelines to surgical precision regarding the environment in which a patient recovers. The rules mandate a minimum area of 400 square feet per 10 beds for Inpatient Departments (IPD), a move specifically designed to eliminate the cramped, dormitory-style living conditions that have characterized many lower-end facilities. Furthermore, centers must provide dedicated rooms for counseling and outpatient services, measuring between 130 and 150 square feet, to ensure that the psychological component of recovery happens in a dignified, private setting. In a region where the stigma of addiction is particularly heavy for women, the rules now mandate distinct male and female wards with adequate privacy protections. This is a vital step toward making treatment accessible to the growing number of female users in J&K who have historically been sidelined or feared seeking help due to a lack of gender-segregated care. Additionally, each center must now maintain at least two beds specifically for emergency stabilization or detoxification, ensuring that patients in the throes of acute withdrawal have immediate access to medical intervention under continuous supervision.
The “medical minimum” established by these rules represents a high bar that will likely force a consolidation of the industry. The administration has recognized that addiction is not merely a social or moral issue, but a complex clinical condition. As such, each center is now legally required to employ at least one clinical psychiatrist, one medical officer, and a clinical psychologist for every 15 patients. The nursing ratio has been set at one nurse for every 10 patients. Beyond the clinical staff, the rules require social workers, record keepers, security personnel, and even dedicated sanitation workers and cooks. This staffing mandate ensures that the “rehabilitation” provided is holistic. It moves the needle from simple containment—keeping a user away from drugs—to active treatment involving cognitive behavioral therapy, medical detoxification, and social reintegration. For many smaller NGOs and private operators, the cost of hiring this level of specialized staff will be significant, but the government’s stance is that the lives of the vulnerable cannot be bartered for lower operational costs.
In a landmark move toward digital surveillance and patient safety, the government has introduced the Unique Treatment Identification Number (UTIN). This system is designed to create a digital footprint for every individual entering the rehabilitation system. Linked to a central database, the UTIN will allow the Licensing Authority to track a patient’s journey across different centers, preventing the phenomenon of “doctor shopping” where patients or their families move from one clinic to another to secure multiple prescriptions for substitution therapies. Before a center can initiate any form of substitution therapy, such as Buprenorphine or Methadone, they must now verify the patient’s treatment history through the government portal. This ensures that the medical intervention is consistent and prevents the diversion of controlled substances—a major concern in a region where the very drugs used to treat addiction have sometimes found their way back onto the black market.
The dispensation of these drugs is now under a microscope. The rules state that drug dispensation must occur under direct clinical supervision, and any “take-home” doses require written approval from a psychiatrist. Centers are mandated to maintain daily dispensing registers, stock registers, and digital entries, all of which must be retained for at least five years. To oversee this, each facility must establish an internal Quality-Assurance Cell. This cell is responsible for ensuring correct dosages, checking for expired medications, and ensuring the proper storage of controlled substances. This layer of internal audit is backed by a severe reporting requirement: any adverse drug reactions must be reported within 48 hours to the Licensing Authority and the Pharmacovigilance Cell. In the most tragic circumstances—the death of a patient or a serious adverse event—the center has a window of only 24 hours to notify the nearest police station, the Chief Medical Officer, and the licensing authority. This level of transparency is intended to dismantle the “hush-up” culture where deaths in custody were sometimes written off as natural causes without proper investigation.
To ensure that these rules are not merely “paper tigers,” the administration has constituted a high-level monitoring committee at the Union Territory level. This body brings together a multi-agency shield comprising representatives from the Health & Medical Education Department, Law, Justice and Parliamentary Affairs, Social Welfare, and the Police (Narcotics). This committee has the power to review the performance of every licensed center and ensure they are complying with the Standard Operating Procedures (SOPs) issued in 2022, alongside WHO and NACO protocols. The Licensing Authority has been granted the power to suspend or cancel a license the moment a center is found to be violating the Act, misusing drugs, maintaining false records, or jeopardizing the safety of its inhabitants.
As the six-month grace period begins, the rehabilitation sector in Jammu & Kashmir stands at a crossroads. For the families who have spent their life savings on substandard care in hopes of saving their children, these rules offer a glimmer of structural hope. For the operators, it is a call to professionalize or perish. The 2026 Rules are a declaration that while the government welcomes private partnership in the fight against drugs, it will no longer tolerate the exploitation of the addicted. By framing these guidelines under the NDPS Act, Jammu & Kashmir has finally aligned its rehabilitation strategy with international medical standards, treating the drug epidemic not just as a law-enforcement challenge, but as a public health emergency that demands the highest level of clinical integrity. The journey from addiction to recovery is long and arduous, but for the first time, the path is being paved with clear, enforceable, and humane rules. (With Inputs from KNO)
Leave a Reply